- DLIM's Playbook
- Posts
- Turf Toe - Joe Burrow
Turf Toe - Joe Burrow
Devin Limerick
October 20th, 2025
Good Morning! happy Monday! The first Friday of the week. Today I’m bringing information on Turf Toe. Something that has sidelined Joe Burrow and put him in the IR list. Whether you’re interested in the rehab or wondering about your fantasy team this will be a good newsletter to read!

Turf Toe is an injury of the first metatarsal phalangeal articulation, due to hyperextension which leads to damage to the plantar capsuloligamentous complex. Which basically means, your big toe bends upward too far causing injury to the ligament underneath the ball of your foot.
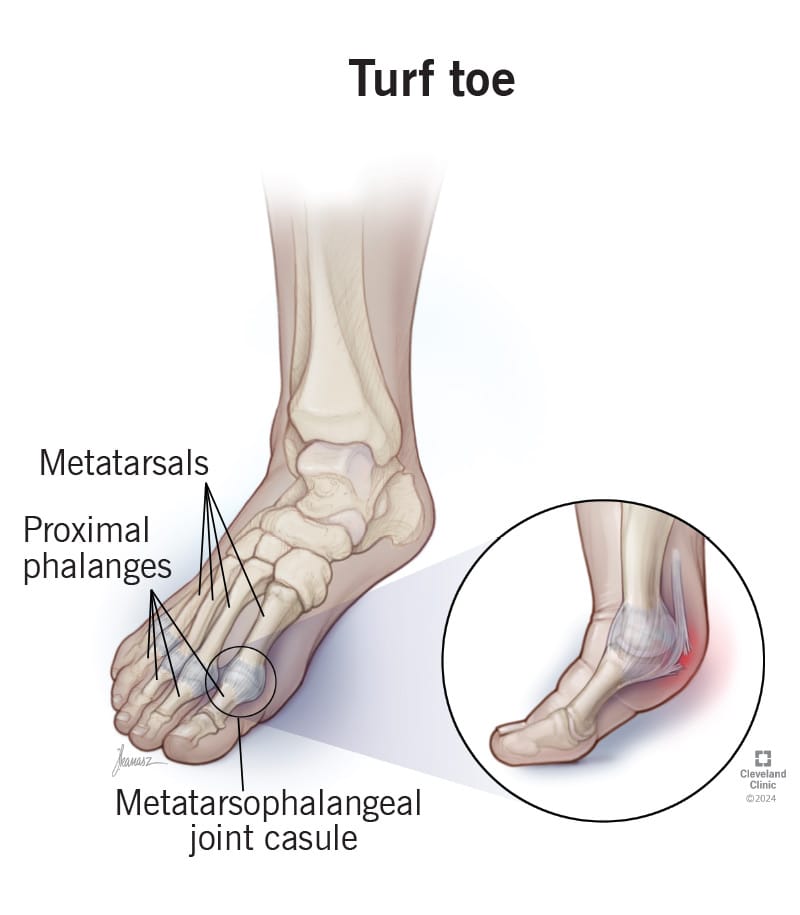
Turf toe is a common injury among football players because of the way the sport demands explosive movements, quick direction changes, and powerful push-offs from the toes. These motion overstretch or sprain the ligaments and capsule surrounding the metatarsophalangeal (MTP) joint at the base of the big toe. Artificial turf, which is less forgiving than natural grass, increases the risk since it doesn’t absorb impact as well and provides more traction, preventing the foot from sliding when it should. Over time or from one major incident, this can lead to pain, swelling, and limited push-off strength.
Turf tow can be categorized into 3 different grades. Grade I can be characterized as swelling in the area, stretching of the plantar ligaments, and minimal redness. Grade II can be characterized as moderate swelling, partial tear of the plantar ligaments, and restricted motion due to pain. Lastly a grade III strain presents with swelling and redness, total rupture of the plantar ligaments, weakness of big toe flexion, and instability of that joint.
In Joe Burrow’s case, it was a grade III which required surgery.

Rehab after turf toe surgery for a quarterback like Joe Burrow focuses on gradually restoring motion, strength, and explosive power while protecting the repaired joint. In the early phase (weeks 0–4), the toe is usually immobilized in a boot or cast to allow soft tissues to heal, with gentle range-of-motion exercises introduced once cleared by the surgeon to prevent stiffness.
From weeks 4–8, physical therapy progresses to light manual mobilization, toe flexion and extension exercises, and balance training to reestablish control through the forefoot. As swelling subsides, strengthening work ramps up—using towel scrunches, marble pickups, resisted toe curls, and calf raises to rebuild intrinsic foot and lower leg stability. This is the hypertrophy phase where we build up strength in the muscles around the injury
Around the 8–12 week mark, Burrow would transition into low-impact conditioning like cycling and pool running before moving to controlled field drills emphasizing push-off mechanics and proprioception. This could potentially be introduced earlier as long as he meets certain criteria to progress to this phase.

In the final phase, explosive movements such as sprint starts, single-leg hops, and cutting drills are reintroduced to mimic game demands, with taping or carbon fiber inserts used to limit excessive toe dorsiflexion. A full return to play often takes 4–6 months, ensuring the joint is strong, pain-free, and stable enough to handle the forces of planting and throwing off the back foot under pressure. However, in Joe Burrow’s case, with all the resources he has and his job to specifically take care of his body, it could take only 3ish months.